Healthy Skeptic
André Picard eschews the hype, pandering and pseudo-science that plague his beat
The sun isn’t up yet, but André Picard is scrolling through Twitter. Most days, he’d be on a 70-minute run up Montreal’s Mount Royal and back to his house in Le Plateau. But Monday is a rest day. That gives the Globe and Mail health columnist more time to read and tweet stories to his over 40,000 followers. This morning, Twitter’s favourite topic is many people’s favourite breakfast food: bacon.
The International Agency for Research on Cancer, the World Health Organization (WHO)’s source for cancer information, has reviewed more than 800 studies about processed meat. The headlines are alarming. “Processed meat joins tobacco, asbestos on WHO list of carcinogens,” proclaims the Globe. “Cancer risk rises with the consumption of bacon, sausage, processed meat,” the Toronto Star warns. Reporters repeat the press release numbers: eating 50 grams of processed meat—about two slices of bacon—daily increases the risk of colorectal cancer by 18 percent. Readers take away three words. Bacon. Causes. Cancer.
After an editor asks him to address the furor, Picard takes his laptop into the Globe’s Montreal bureau on the 16th floor of a downtown office building. Flanked by the pieces of his unused desktop computer and a view of shiny skyscrapers, he calmly and efficiently does what he always does: writes a column based on research, clear thinking and logic. By 1 p.m., it’s on the Globe’s website. The headline: “Go ahead, have that BLT for lunch.”
Many other journalists committed a common error. Eighteen percent is the relative risk, a comparison between those who eat processed meat and those who don’t. The more representative numbers are the absolute risk: 56 out of 1,000 non-processed meat eaters will develop colorectal cancer anyway; for bacon aficionados, that number goes up to 66. Hardly worth overhauling your diet. The WHO released a clarification three days later, and many news outlets published follow-up stories with a more measured approach to the science. But Picard didn’t need the new press release to get it right.
When journalists get health stories wrong, the consequences can be dire. After the U.S. Food and Drug Administration warned in 2003 and 2004 that antidepressants may cause suicidal thoughts in young people, the overblown coverage changed public perception dramatically. Parental fears led to fewer young people with depression getting treatment, and a 2014 British Medical Journal study found an increase in suicide attempts.
Health journalism also has to counteract junk science and misinformation. The anti-vaccine movement, for example, puts belief over evidence, endangering everyone else’s health. Meanwhile, celebrities peddle pseudo-science: Gwyneth Paltrow is devoted to “detoxifying” juice cleanses, and Demi Moore attempted to clean her blood with leeches. But too often, reporters are the ones who get the science wrong. Picard, who’s been writing about health for almost 30 years, fights the misinformation every day. On the page, he is an assertive advocate for good health policy; in person, he’s soft-spoken, kind and genuine, with a dry wit that reveals itself slowly. His strong statements sometimes make people—doctors, activists or politicians—look bad, and they get angry, yet he’s almost universally respected and well-liked. Although Picard and many other full-time health reporters have the time to do it well, the beat is easy to screw up. General assignment reporters and new journalists can make common mistakes—hyping new discoveries, pandering to emotion or just plain getting the science wrong—that lead to false hope, dangerous health decisions and widespread misunderstandings.
Now 55, Picard stumbled into journalism at the University of Ottawa, which has both French and English student papers. He joined the English paper, The Fulcrum, despite being a francophone born in Ottawa and raised in North Bay, Ontario, because it was looking for a record reviewer. He then worked on the business side, putting his accounting major to work. By the time he graduated, he’d served as both arts editor and editor, which led to two years working for the Canadian University Press. After doing Carleton University’s one-year journalism program, he moved to Toronto to intern at the Globe. While there, he reconnected with his future wife, Michelle Lalonde, whom he knew at The Fulcrum (she’s now a reporter at the Montreal Gazette).
In 1988, the Globe sent him to Toronto’s St. Michael’s Hospital to investigate a mistreated patient. When he arrived, he found a sign warning others to stay away, implying that the man, who was gay, posed a high risk of contamination. Picard introduced himself to the patient and reached out to shake his hand. The patient took it and burst into tears—he hadn’t been touched in days. The reason he was being treated: a urinary tract infection. Titled “Gay patient angered by AIDS warning card,” the story gave its stigmatized subject a voice. “He said he was humiliated by the experience and appalled by the ignorance of medical staff regarding AIDS and homosexuals,” Picard reported. “‘I had visions of the Nazis when I saw that sign. It was as if I was branded with the pink triangle,’ he said.” According to Picard, on the morning the story came out, the sign came down, and the hospital apologized.
Picard continued covering AIDS after he moved to the Globe’s Montreal bureau in 1989. “Writing early and a lot about AIDS is what changed my perception of health being not just medicine, but a very political issue,” he says. Like any new reporter, he made mistakes while starting out. In a 1987 story about a liver cirrhosis drug, for example, he erred the way other reporters did on the bacon story: he cited the more dramatic relative mortality numbers instead of the absolute risk. When he misstepped, readers wrote and phoned, and he learned.
“A wonder drug’s dark side,” declared the front-page headline in the Star on February 5, 2015. The story, by the paper’s investigative team, was about young women who said they had adverse reactions to the Gardasil vaccine, which reduces the risk of some cancer-causing forms of HPV. “Since 2008 at least 60 girls and women in Canada have convulsed or developed disabling joint and muscle pain and other debilitating conditions after receiving Gardasil,” wrote David Bruser and Jesse McLean. “One needed a wheelchair, another a feeding tube. A 14-year-old Quebec girl, Anna- belle Morin, died two weeks after receiving the second injection of the vaccine.” Ardent anti-vaxxers championed the article.
One problem, though. The journalists messed up a fundamental principle of science: correlation is not causation. The anecdotes don’t reflect the overwhelming evidence that the vaccine is perfectly safe. Just because two things happen doesn’t mean they’re related to each other. The story mentioned the lack of proof only in the 11th paragraph: “In the cases discussed in this article, it is the opinion of a patient or doctor that a particular drug has caused a side-effect. There is no conclusive evidence showing the vaccine caused a death or illness.” The Star removed the article from its website 15 days later. “If anyone in the newsroom had consulted with any of the Star’s excellent health and medical reporters,” public editor Kathy English wrote in her column on the story, “they could have explained the inherent land mines in not giving greater weight to scientific evidence.”
Even less dramatic mistakes can cause damage. When the scientific consensus is particularly strong, proposing another opinion is like saying the earth is flat. But journalism thrives on conflict. The “vaccine debate,” for example, is based on the idea that vaccines cause autism, though the scientific consensus is that there is no connection. A 2015 Ottawa Sun story presented the point of view of an anonymous anti-vaxxer: “‘We are not part of a herd,’ said the mother. ‘We are rational, intelligent human beings who can make informed decisions of how to obtain and maintain a healthy lifestyle.’” That same month, CBC Radio’s The Current interviewed parents on both sides, giving both a platform to share their views. Listening to anti-vaxxers without debunking their beliefs suggests vaccination is something up for debate. According to the science, it’s not.
Covering only individual studies also creates distortions. Health reporters receive a flurry of press releases—Kelly Crowe, medical sciences correspondent for CBC National News, gets up to 50 a day. Each study is embargoed, so most stories come out at the same time. “It creates a false sense of something happening,” Crowe says. “Science evolves, and news has to happen, and there’s an inherent contradiction there.” Studies with opposing results are a normal part of the scientific process: over time, consensus emerges. But reporting on each one along the way leads to contradictory headlines: a proclamation that chocolate is good for you one day and a warning that it’s bad the next.
Crowe is thankful she works on stories about broader issues instead of just reporting on the newest studies and technologies. “Because what are the real determinants of health?” she asks. “They’re poverty, they’re education, opportunities, geography.” But these issues aren’t news to some editors; nor are research funding and broader health policies.
Sensationalism is another trap. Timothy Caulfield, a health and law professor at the University of Alberta, has researched hype in the beat. Some news stories about scientific studies inflate benefits, but few discuss costs or potential risks. He calls this “hype by omission”: if readers learn only the possible benefits of a new drug or treatment, they’re left with false hope.
The balance is hard to get right, and even Picard is not immune. In 2009, Italian doctor Paolo Zamboni’s research on his proposed multiple sclerosis (MS) treatment, which involved clearing blocked or narrowed veins in the neck, found improvements in the patients. In a companion feature to a CTV documentary, Picard described Zamboni’s results as “stunning” and “striking,” though he added the caveat that the evidence was “too scant and speculative to start rewriting medical textbooks.” He now says the challenge facing the documentary team—which did the research—was that the study’s skeptics were unwilling to comment. The result was a one-sided story.
Patients demanded governments pay for clinical trials to “liberate” the veins and even travelled to other countries for the unproven treatment. In 2010, a man died after undergoing the procedure in Costa Rica. But Zamboni’s study was not a double-blind randomized controlled trial, the gold standard for scientific experiments (see sidebar on page 43), and tested only 65 patients. Further studies found little difference between the neck veins of people with MS and healthy control subjects, meaning Zamboni’s theory might not be as stunning as the stories suggested.
The good news is health journalism, like science, is self-correcting. Picard’s subsequent work on the topic was much more skeptical. “The saga is also a sobering reminder that, as much as we yearn for simple solutions, they rarely exist,” he wrote in 2010. But the initial article remains on the Globe’s website without a correction. And general assignment reporters rarely have the same second chance to get it right.
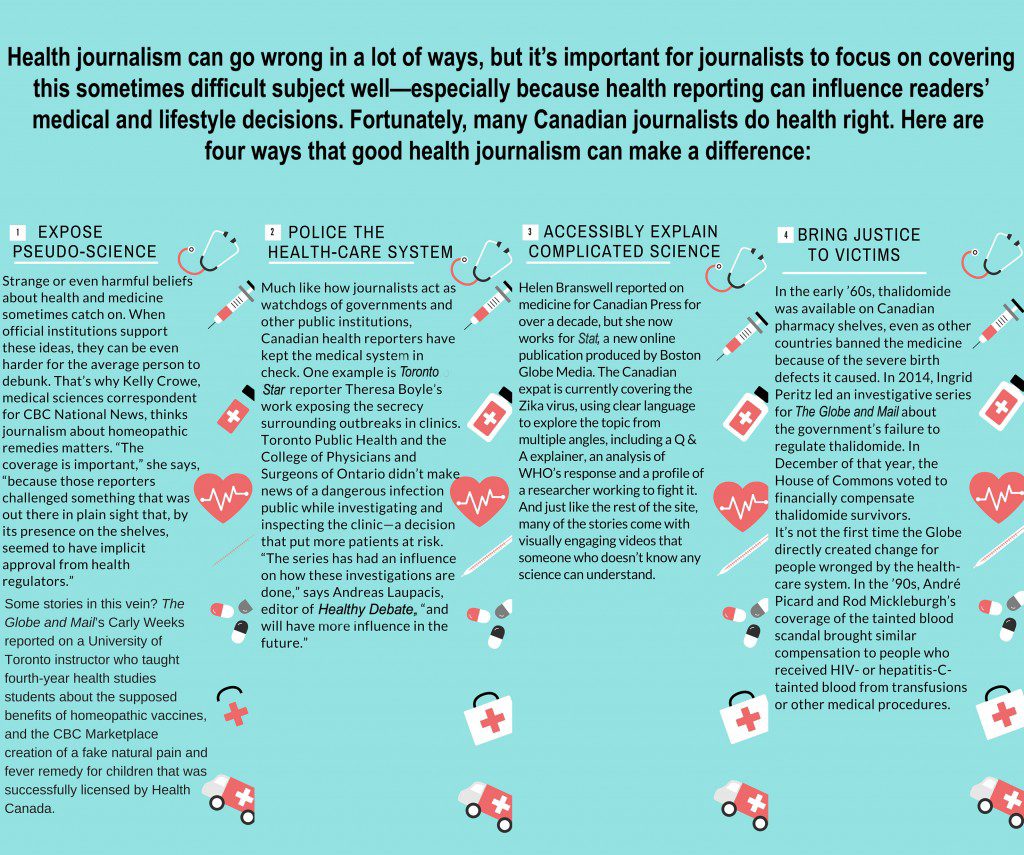
Read stories by Carly Weeks, Theresa Boyle, Helen Branswell and Ingrid Peritz
“I killed my son,” the email begins. That gets Picard’s attention. He goes on to read a heart-wrenching story from a B.C. woman who’d been left alone with her newborn son in the hospital. She fell asleep, rolled over and asphyxiated her baby. Hospital staff told her he had died of sudden infant death syndrome; she didn’t learn the real story until months later, while reading the coroner’s report.
Picard calls her but isn’t convinced that he should tell her story. “When you write about these really personal issues, which I often do, you worry about what the impact’s going to be on the person,” he says. But he kept talking to her over several months, until a larger story emerged. “The perils of sharing bed with baby” became a front-page feature. The woman’s story is the lead of a 1,400-word article that explores how to do co-sleeping correctly. He wrote it in his typical style—clear, with specific examples: “The baby should always sleep on his back, on a hard surface: no waterbeds, no makeshift beds made of cushions or pillows, and no sleeping on the couch or in the Laz-E-Boy.”
Not all journalists show such restraint. In 2011, when Ontario refused to pay for a $40,000 cancer drug for a mother of two, reporters dialled up the despair. The Globe’s Lisa Priest present- ed it as an injustice: “All the best medical advice could not have prepared a 35-year-old breast cancer patient for this: After finding a lump, Jill Anzarut was told her tumour was ‘too small’ to be treated with a drug that can prevent a recurrence, potentially saving her life.” Matt Gurney of the National Post wrote, “Ms. Anzarut, by catching her cancer early, disqualified herself from the best possible treatment.”
Few stories mentioned the drug’s potential side effects— including heart failure, lung damage and increased risk of infection—or that the researchers didn’t test tumours as small as Anzarut’s. Evidence-based or not, the whirlwind of stories created enough political pressure that the province paid for the drug. The Star’s Theresa Boyle says such situations benefit only the individual in the news, not the system or anyone in the same situation. She once received a call about a young boy who would go blind without a costly U.S. operation that Ontario wouldn’t fund. “When you write up stories like this, they can result in the person getting the treatment they want,” she says. “Is that fair to all the others who have been turned down for treatment?” She chose not to cover the story, but another Star reporter wrote it after the issue was raised in question period at Queen’s Park.
These pieces often fail to mention why drugs can be so expensive: drug companies looking to make a profit. Research and development are often covered by grants and publicly funded universities, so astronomical sticker prices aren’t just for covering the manufacturing costs. But instead of including drug pricing in the discussion, some journalists go for the heartstrings. Reporters unfamiliar with the beat are at a distinct disadvantage because there’s so much to know, including the scientific consensus on a topic, how Canada’s health system works and what makes a good study. And in a modern newsroom, many health stories go to general assignment reporters.
But journalists are only part of the problem. “A lot of the actual hype flows from what we call the hype pipeline,” says Caulfield, “where build-up of exaggeration or misinformation happens.” Researchers, who are under pressure to publish and commercialize their work, may talk up their research in the abstract—the summary at the top of every research paper—which is sometimes the only part of the study reporters read. The press release adds another layer of sensation. In the “bacon causes cancer” stories, for example, the press release reported the relative risk, while only a reporter familiar with health might read the study to find the absolute risk. Then, journalists need to catch their audience’s attention and simplify the science to make it understandable. Next, at newspapers, an editor—usually without a scientific background—writes the headline. “In each one of these steps, there are complicit collaborators,” says Caulfield. “Everyone benefits along that chain from a little bit of hype.”
Meanwhile, many scientists are more comfortable with jargon and the specialized knowledge of their field than with plain language. Terms like metastasized, derma, biopsy or clinical trial may confuse reporters, who must ask for explanations or risk leaving readers even more confused.
And editors push for stories they think readers want: diet tricks, waiting room times or the annual article on how bad the allergy season is (despite data suggesting otherwise). Maureen Taylor, Crowe’s predecessor at CBC, left full-time journalism to become a physician assistant (although she’s on the editorial board of Healthy Debate). One reason for the career change was her frustration with superficial daily health reporting. “Often what producers and editors think the audience wants are those lifestyle-type stories,” she says, citing “bacon causes cancer” as an example of what tops newscasts. “But it’s not going to be the story that you’re proudest of.”
The moderator reading Picard’s bio pauses to take a breath, and one of the 30 or so health professionals and reporters in the room starts to clap. Everyone laughs when the moderator adds more accomplishments to the list. When he gets to the podium, Picard smiles and quips, “Yeah, my mom sends those long emails to everybody.”
He’s at a Toronto YMCA for a panel about the benefits and harms of covering suicide; Picard is the only journalist, speaking along with three health professionals. His stage persona is similar to how he is on the page: blunt, clear and based on evidence. Picard’s also the only speaker to get multiple laughs. He’s well practiced; speeches and talks on everything from patient-centred care to psychology are a regular part of his schedule. About half of these gigs are paid, but he expresses his honest opinions as a columnist, occasionally disagreeing with the experts who invited him. At the Y, he says journalists are unlikely to ever follow suicide reporting guidelines created by outside agencies like the Canadian Psychiatric Association, such as to “avoid exciting reporting,” and refrain from publishing photos of the deceased.
In the Q & A portion, a man asks about Picard’s suggestion that a health reporter would write differently about suicide than someone on the crime or arts beat. “What do we do about that?” the man asks. Picard responds, “What we do is have breakfasts like these for crime reporters instead of health reporters.”
Kathryn O’Hara, CTV chair in science broadcast journalism at Carleton, is also a proponent of education. Even six weeks of science training in journalism school—especially understanding statistics and research evaluation—would help young reporters get health stories right as general assignment reporters.
Gary Schwitzer, publisher of HealthNewsReview, thinks the checklist his blog’s expert reviewers use could be a good guideline for journalists. Up to 70 percent of stories they analyze miss items such as discussing costs or quantifying downsides. But there’s still reason for optimism, he says, because “there are lots of unprecedented peaks of excellence”: journalists who write about health well. “Unfortunately,” he continues, “those peaks of excellence have in between them a wider and deeper valley of this day-to-day tsunami of garbage.”
Picard is a peak. “One thing about working with André is that it really humbles you,” says Paul Taylor, Globe health editor from 1998 to 2013. “Whatever you think about your own skills, André is so much better.” Taylor once asked Picard to write a column a half-hour before deadline; it came in exactly to word count. “He wrote the story faster than I could just type it.” Les Perreaux, the Globe’s Montreal bureau chief since 2010, was intimidated by Picard when he started the job. “But it didn’t take long to realize that he’s actually a very nice guy, a very generous colleague and a good lunch mate.”
Jeremy Petch, managing editor at Healthy Debate, says Picard is well respected across the health care system. “People read him whether they agree with it or not.” And sometimes, they really don’t agree. Last October, Picard wrote an op-ed about doctors’ “sense of entitlement.” He was reacting to a dispute between the Ontario Medical Association (OMA) and the province, which cut physicians’ fees. (The OMA has since launched a charter challenge against the province.) Doctors can legally strike but face restrictions because they provide an essential service. Instead, the physicians started a social media campaign. Picard took issue with the tone and content of their tweets. He wrote: “There’s a fine line between warning and threatening reductions in patient care, and between highlighting your hard work and whining about your workload and, too often, physicians have veered to the wrong side of that line.” He argued for binding arbitration.
Many doctors felt insulted, and they let him know—directly and on social media. Merrilee Fullerton, a retired Ottawa-based family physician, says, “I think what was really noticeable to me was the word ‘entitlement.’” She accuses Picard of approaching stories with his mind made up—in this case, “his bias is that physicians are probably overpaid, do not require the respect they have traditionally been given, that other people can do their jobs and that they are essentially greedy.”
Such accusations don’t bother or surprise him anymore. What does bother him, though, is people attributing thoughts and statements to his column that he didn’t actually write. He often retweets criticism with a correction.
Flak from both sides of an issue shows that Picard is balanced, says Taylor. During his time at the Globe, he sometimes had trouble explaining what Picard was writing about at editorial meetings, because he wasn’t sure what side of an issue the columnist would come down on. “That’s partly because he isn’t ideological,” Taylor says. “He’s evidence-based, and unless you know what the evidence says, it’s hard to know what he’ll say.”
The evidence was on Picard’s mind in February 2015, when hockey legend Gordie Howe seemed to bounce back from a severe stroke after an experimental stem cell treatment in Tijuana, Mexico. Many reporters, especially in sports sections, quoted the Howe family’s description of the treatment as a “miracle” without question. But an important caveat was missing. Stem cells, building blocks that can transform into specialized cells, are our bodies’ built-in repair system. They can successfully treat some diseases, like leukemia, but there’s no evidence that they can fix post-stroke brain damage. Suggesting otherwise could push desperate people to try risky and expensive options.
Picard wrote that one anecdotal success story is not evidence that these treatments work. He also pointed out holes in other reporters’ narratives: not mentioning the brain’s capacity to rewire itself after a stroke and Howe’s occupational, physio and speech therapy that could have contributed to his improvements. “The media coverage of Mr. Howe’s ordeal,” Picard wrote, “more than anything else, is a striking example of how science should not be presented to the public.”
To be consistent and get things right, Picard relies on lots of reading, learning and meeting experts at conferences. He calls far more experts than he quotes, just to make sure that his assumptions and thinking are in line with the evidence. “To me,” he says, “the guiding force is just try to be fair.” In other words, health reporters have the same responsibility as everyone else in the newsroom: to do good journalism.